Collagen cross linking (CXL) is a procedure recommended more and more to those with keratoconus and other corneal degenerative conditions. Although it is not intended as a cure, ie it is not a treatment designed to affect a change in the corneal shape it does significantly slow or stop the progression of the disease in the majority of those treated.
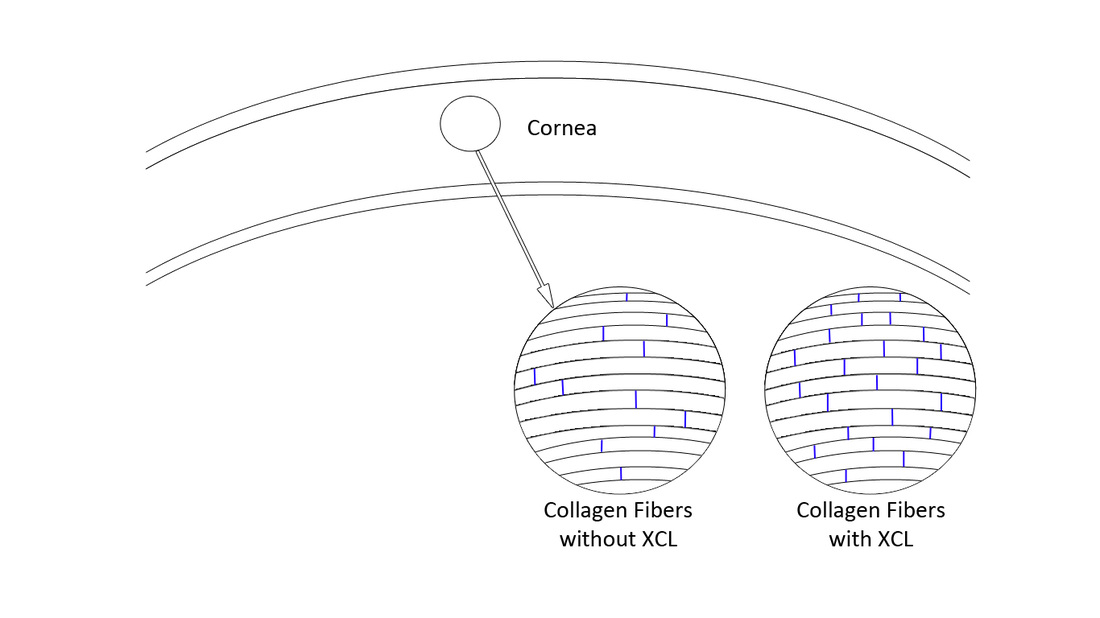
The cornea is soaked in Riboflavin and when this is activated with UV light it causes the collagen fibers that make up the cornea to create stronger bonds to each other, therefore, strengthening the tissue hence halting the progression of the keratoconus.
CXL is definitely recommended where progression is noted in patients with corneal ectasia, however, more and more surgeons are now recommending it regardless of this evidence, especially if the patient attends at a younger age ie under 22. This is because of the high rate of success and relatively low risk involved with the procedure but also the potential to halt the progression of the disease. It cannot be performed, however, on those eyes where the cornea has advanced ectasia and has become too thin, typically to below 400 microns, although this would be decided on a case by case basis.
In older individuals the cornea becomes naturally cross linked due to the build up of UV exposure from the dun. This is why Keratoconus generally ceases to progress after the age of 30.Therefore, it is unlikely to be necessary in patients of this age and above, however, at least an annual check-up is recommended to make sure that the cornea has stabalised.
The cornea is soaked in Riboflavin and when this is activated with UV light it causes the collagen fibers that make up the cornea to create stronger bonds to each other, therefore, strengthening the tissue hence halting the progression of the keratoconus.
CXL is definitely recommended where progression is noted in patients with corneal ectasia, however, more and more surgeons are now recommending it regardless of this evidence, especially if the patient attends at a younger age ie under 22. This is because of the high rate of success and relatively low risk involved with the procedure but also the potential to halt the progression of the disease. It cannot be performed, however, on those eyes where the cornea has advanced ectasia and has become too thin, typically to below 400 microns, although this would be decided on a case by case basis.
In older individuals the cornea becomes naturally cross linked due to the build up of UV exposure from the dun. This is why Keratoconus generally ceases to progress after the age of 30.Therefore, it is unlikely to be necessary in patients of this age and above, however, at least an annual check-up is recommended to make sure that the cornea has stabalised.